Divergent propagation
Energy is distributed radially from the contact point, without focusing at depth.
Professional radial shockwave therapy system

Adjustable pressure
Pressure of up to 7 bar for individualized, precise treatment settings.
Working frequency
Range of 1 to 21 Hz to match the pulse rate to the clinical protocol.
Specialized applicators
A broad range of applicators for specific anatomical areas and therapeutic goals.
Maximum output energy
Controlled energy delivery for precise, reproducible application.
Use the Previous and Next buttons or keyboard navigation to view the photos.
A non-invasive approach for managing superficial musculoskeletal conditions, myofascial syndromes, and overuse-related disorders.
Radial shockwave therapy is used mainly for superficial soft-tissue conditions, myofascial pain syndromes, and overuse-related musculoskeletal conditions. Its clinical use is documented in the management of plantar fasciitis, tendinopathies, certain muscle injuries, and trigger points.
However, radial technology is not designed to penetrate deeper tissues or to treat intra-articular conditions. Even at high energy levels, radial therapy remains a surface-oriented treatment modality.
A review of the publicly available technical documentation from the leading manufacturers of radial shockwave systems shows that much of the material is geared primarily toward marketing communication and offers limited physical or engineering detail. This is partly because radial technology is now highly mature and, in its basic structure, comparatively simple.
The fundamental physics of radial wave generation has remained essentially unchanged for more than 20 years: pneumatic or electromagnetic energy generation, mechanical impact on the applicator, and propagation of a diffuse radial wave.
The effective penetration depth of radial waves is physiologically limited and generally does not exceed 0.8-1.6 in (2-4 cm). As a result, the clinical outcome depends largely on the experience of the physician or physiotherapist, the correct selection of parameters, and the application technique, and less on the nominal values listed in the device specifications.
Even at energy levels of 200 mJ, radial shockwave therapy retains its predominantly superficial character. Radial waves propagate from the applicator contact point, have no focal point, lose energy continuously as depth increases, and are clinically effective mainly within a penetration depth of about 0.8-1.6 in (2-4 cm).
An applied energy of up to 200 mJ is a high value for radial therapy, but it does not equate to the therapeutic properties of focused shockwave therapy.
The practical differences between radial systems lie not primarily in the advertised pressure or energy values, but in operational characteristics that influence treatment reproducibility.
Energy is distributed radially from the contact point, without focusing at depth.
The main clinical effect involves superficial soft tissue, the fascia, the muscles, and peritendinous structures.
The outcome depends on the operator's experience, the selection of parameters, and the quality of tissue contact.
RSWT stands for radial shockwave therapy and FSWT for focused shockwave therapy. Radial technology is a mature, non-invasive, and versatile solution for superficial soft tissue, whereas focused technology is designed for deeper structures and specific orthopedic applications.
In practice, the most significant differences between radial systems involve pulse stability, mechanism service life, ergonomics, the range of applicators, and the predictability of results under real clinical conditions.
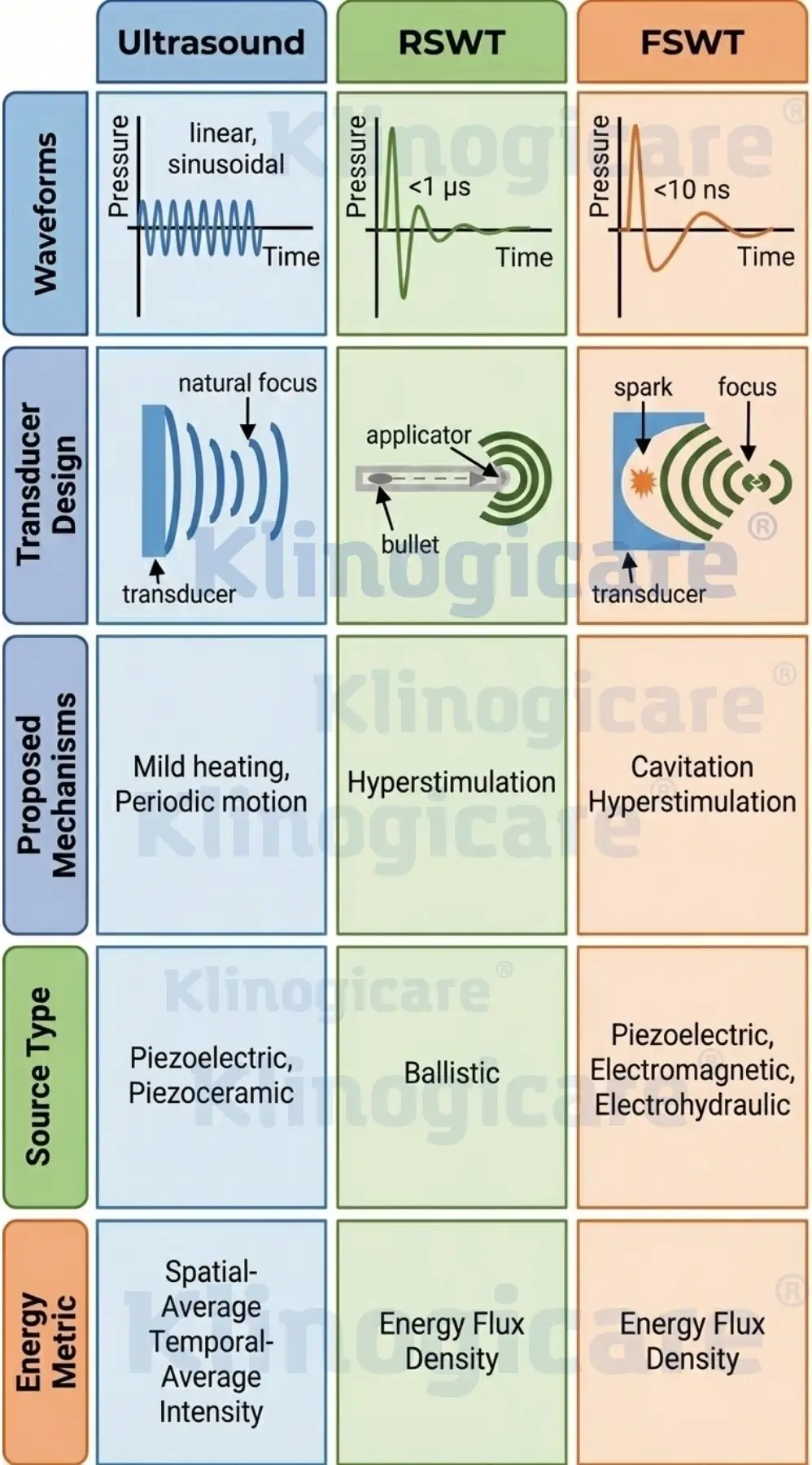
To properly evaluate a shockwave system, it is important to distinguish the physical parameters used across the different technologies and to understand what they actually measure.
In ultrasound devices, SATA indicates the average ultrasound power, calculated over both the transducer surface and the entire exposure time, including the pause intervals between pulses.
Shockwave therapy is not a simple vibration but a succession of short, high-pressure pulses. EFD indicates the amount of energy applied per square millimeter at the point of impact or, in focused systems, at the focal point.
Ultrasound consists of rapid, relatively continuous vibrations that act gradually over time, which is why average power is measured. Shockwaves, by contrast, are instantaneous high-energy pulses: here the energy density of each impact event as it penetrates the tissue is more relevant.
Unlike focused systems, radial therapy lacks standardized, tissue-referenced values that would allow a comprehensive quantification of absorbed energy, depth distribution, or attenuation profiles.
At present there is no commonly accepted criterion for quantifying absorbed energy, energy distribution as a function of depth, or attenuation profiles in radial therapy that is comparable to the criteria applied to laser or ultrasound technologies.
A useful differentiation between radial systems should not be based on nominal values, but on operational and biomechanical characteristics that influence clinical outcomes.
The clinical efficacy of radial therapy is determined not only by the device specifications, but by the interplay between system performance, parameter selection, and operator technique. Stability, reliability, and predictability of energy delivery are therefore key factors in physiotherapy and sports medicine practice.
Rather than historical tradition or abstract performance claims, the evaluation should be based on the system's ability to function as a practical, reproducible, and predictable clinical tool under everyday working conditions.
| Energy level | Clinical application |
|---|---|
| 60-100 mJ 1-2 bar |
Superficial soft tissue, muscle tightness, myofascial pain, and trigger points. |
| 100-150 mJ 3-4 bar |
Tendinopathies, fascial conditions, and chronic muscle pain. |
| 150-185 mJ 5-6 bar |
Dense fascial structures, chronic degenerative changes, and pronounced pain syndromes. |
Klinogicare® Shockwave Storm Radial is a portable system for radial shockwave therapy, designed for the controlled stimulation of superficial soft tissue. The device emits acoustic pressure waves with adjustable parameters, enabling controlled, reproducible mechanical stimulation of a defined treatment area.
The system generates radial waves through an internal mechanism that accelerates a projectile inside the handpiece. The resulting mechanical wave propagates radially through the tissue and produces mechanical stimulation that may support local microcirculation, pain modulation, and soft-tissue recovery processes.
In clinical practice, the response is usually assessed over a course of several sessions, typically around 3-4 sessions per week. A typical session lasts about 10 minutes and allows for standardized, operationally efficient therapy.
The adjustable pressure and frequency parameters, from 0.5 to 7 bar and from 1 to 21 Hz, allow controlled application for both acute and chronic soft-tissue conditions. The system provides reproducible output and supports a more predictable clinical application, provided it is used with appropriate technique and parameters.
Radial therapy is non-invasive and is generally well tolerated. Transient local reactions, such as mild discomfort or skin redness, may occur, without functional limitations or downtime.
The system is supplied with 13 applicators: 6 for pain indications, 3 for paravertebral areas and regions of vertebral origin, and 4 for fascial and myofascial therapy.
The various shapes and diameters allow work on trigger points, tendon insertions, large muscle groups, and fascial chains.
Applicator selection and protocol recommendations are integrated into the control interface, which reduces preparation time and operator error.
Radial therapy is applied externally, without injections or anesthesia, and is widely used in the management of musculoskeletal and myofascial pain.
No recovery time is required after treatment. In most cases, the patient can resume normal daily activities immediately afterward.
The mechanical action of radial waves may stimulate tissue-healing processes, may improve local circulation, may reduce pain sensitivity, and may support regeneration in subacute and chronic conditions.
Adjustable energy and frequency allow precise dosing of intensity according to the clinical indication and individual tolerance. Before treatment, contraindications should be checked and current clinical guidelines followed.
Shockwave Storm Radial is configured as a professional system for superficial radial applications, with adjustable parameters, treatment protocols, and a complete set of applicators for different anatomical areas.

The appearance of the product may vary depending on the region of supply. The technical and functional specifications are identical across all versions.
This section offers a comprehensive scientific overview: bibliographic references, study images, and full abstracts, useful for physiotherapists, sports physicians, and sports facilities.

The treatment of musculoskeletal conditions in athletes with extracorporeal shockwave therapy is becoming increasingly widespread as the evidence for its use grows. ESWT protocols can be tailored clinically and include energy flux density, the number of pulses, the type of shockwave (focused or radial), the number, frequency, and duration of sessions, the application area, as well as follow-up recommendations.
Protocols vary across studies and, for many indications, the optimal protocols have yet to be defined.
According to the authors, ESWT can be used safely for a range of musculoskeletal conditions in athletes, including rotator cuff tendinopathy, lateral elbow epicondylopathy, greater trochanteric pain syndrome, hamstring tendinopathy, patellar tendinitis, Achilles tendinopathy, other tendinopathies, plantar fasciitis, bone stress injuries, and medial tibial stress syndrome.
ESWT can also be used during the competitive season in athletes, as it often requires little or no break from sport and may provide benefits quickly. It should be combined with physiotherapy to support long-term functional improvements and optimize healing processes.
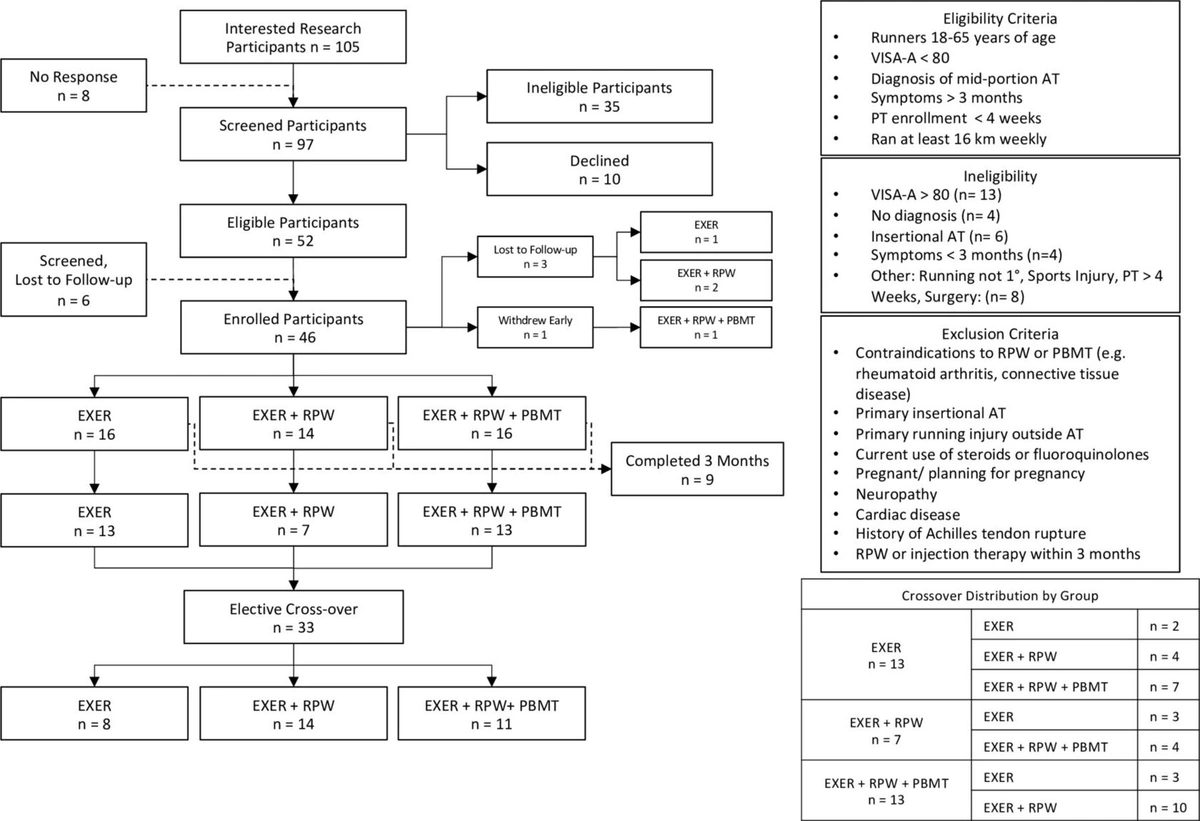
Non-insertional Achilles tendinopathy is a common injury in runners. A progressive loading exercise program is the primary treatment. Other options include radial pressure waves, commonly referred to as shockwaves, as well as photobiomodulation.
The authors hypothesized that exercise plus radial pressure waves, as well as exercise plus radial pressure waves plus photobiomodulation, could achieve a greater reduction in symptoms, measured with the VISA-A scale, and superior functional improvement compared with exercise alone. A secondary objective was to explore outcomes after three additional months of elective treatment.
Runners with Achilles tendinopathy and symptoms present for more than 3 months were randomized into three groups: exercise alone, exercise plus radial pressure waves, or exercise plus radial pressure waves plus photobiomodulation. Radial pressure waves were administered once a week over three treatments. Participants in the photobiomodulation group additionally received two treatments per week for 3 weeks.
The VISA-A, the University of Wisconsin Running Injury and Recovery Index, and the 29-item Patient-Reported Outcomes Measurement Information System were collected at baseline and at successive intervals over 3 months. Runners could then choose another treatment for three additional months.
A total of 46 runners were included, 24 men and 22 women, with a mean age of 40 ± 12 years. At 3 months, runners in the exercise plus radial pressure waves group showed greater improvement than exercise alone on the VISA-A scale, with a mean of 33 versus 18 points, p=0.023; 95% CI: 2.4-28.4.
No differences were observed between exercise plus radial pressure waves plus photobiomodulation and exercise alone, 25 versus 18 points, p=0.12; 95% CI: -10.8-25.9. In the exercise plus radial pressure waves group, greater improvements were seen in running-specific indices, pain interference, and social roles compared with exercise alone.
During the subsequent 3 months of crossover treatment, the VISA-A score increased by 11 points in the groups that switched to exercise plus radial pressure waves and to exercise plus radial pressure waves plus photobiomodulation, both with p<0.05 compared with exercise alone.
The combination of exercise and radial pressure waves showed the greatest measured reduction in symptoms at 3 months. However, all groups achieved clinical improvement, which confirms the importance of exercise. Larger studies in other physically active populations may further clarify the clinical benefits of each treatment.
All players were male, aged between 18 and 35 years. They were professional soccer players from the German first and second Bundesliga.
The study compared the time-loss durations obtained when treating acute muscle injuries in elite soccer players with a multimodal approach, which included a specific protocol of near-daily radial extracorporeal shockwave therapy, with data published in the literature.
The authors carried out a retrospective analysis of the treatments and recovery times of the muscle injuries sustained by players of an elite club during one of the previous seasons.
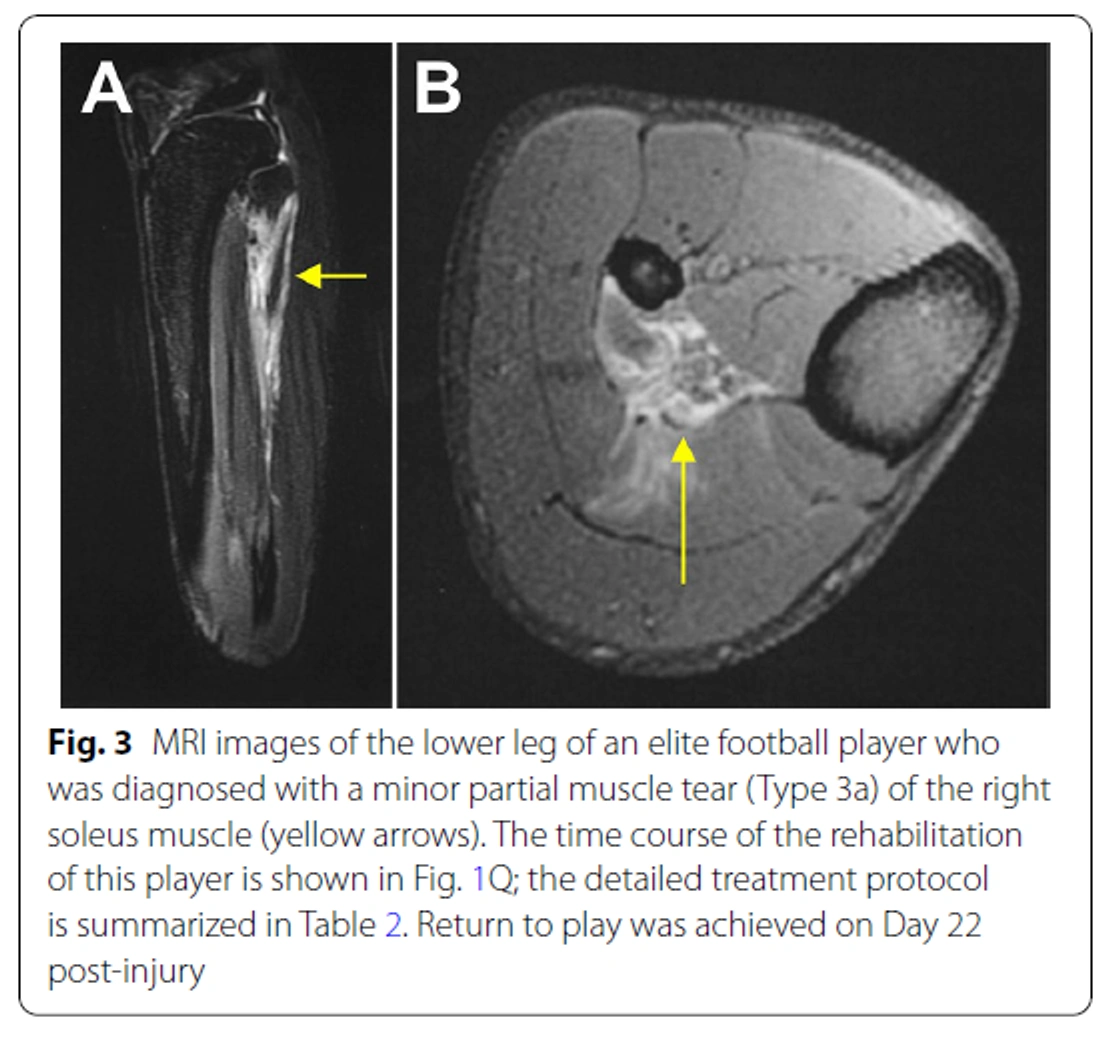
Twenty acute muscle injuries were diagnosed and treated: eight, equivalent to 40%, were classified as type 1a muscle hardening; five, equivalent to 25%, as type 2b muscle fiber tears; four, equivalent to 20%, as type 3a partial muscle injuries; three, equivalent to 15%, as contusions.
All injuries were treated with the multimodal approach described. Compared with the data published by Ekstrand et al., Br J Sports Med 47:769-774, 2013, the median and mean time-loss durations in type 1a injuries were reduced by 54% and 58%, respectively.
Time-loss durations were reduced by 50% and 55% in type 2b injuries, and by 8% and 21% in type 3a injuries. No adverse reactions were observed.
Overall, the multimodal approach evaluated in the study represents a safe and effective strategy for treating acute type 1a and 2b muscle injuries in elite soccer players and may help prevent more serious structural muscle injuries.