Focused ESWT
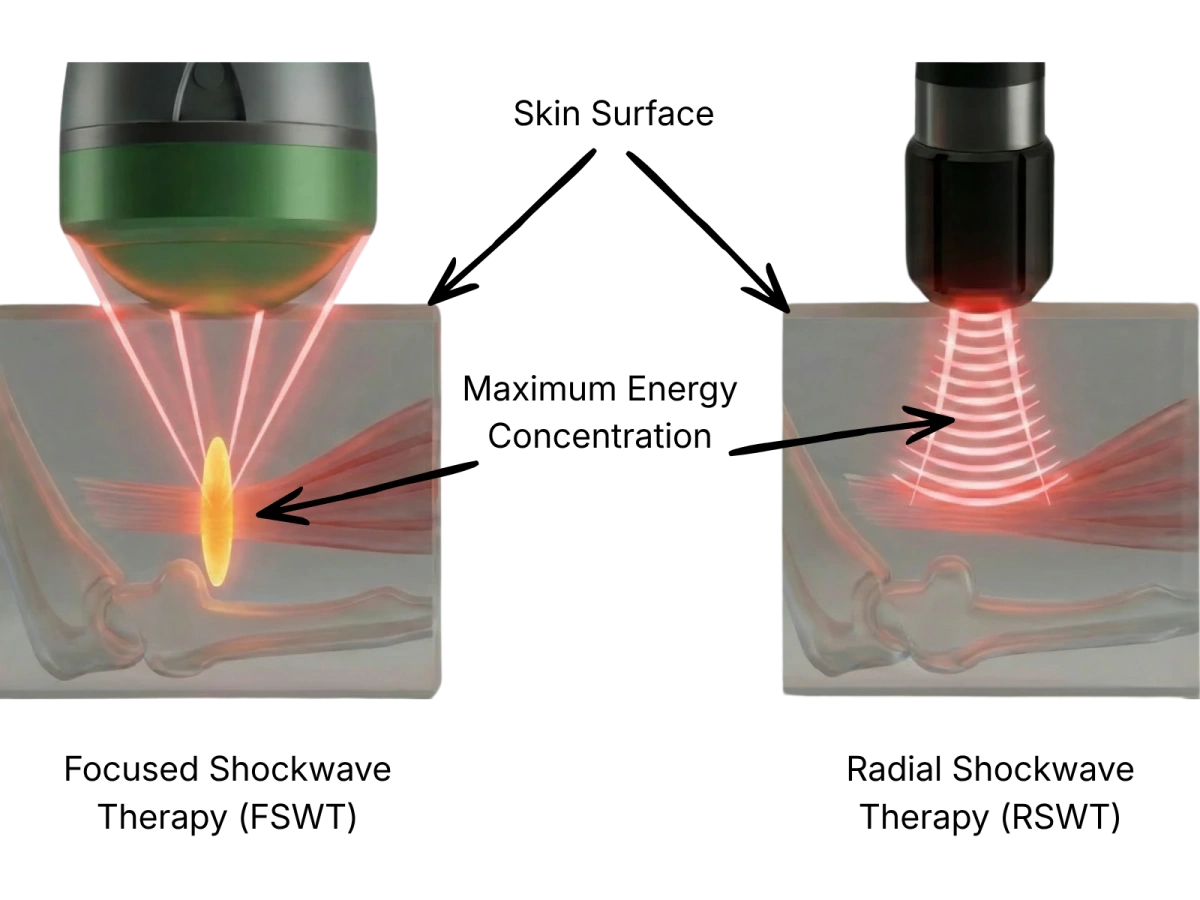
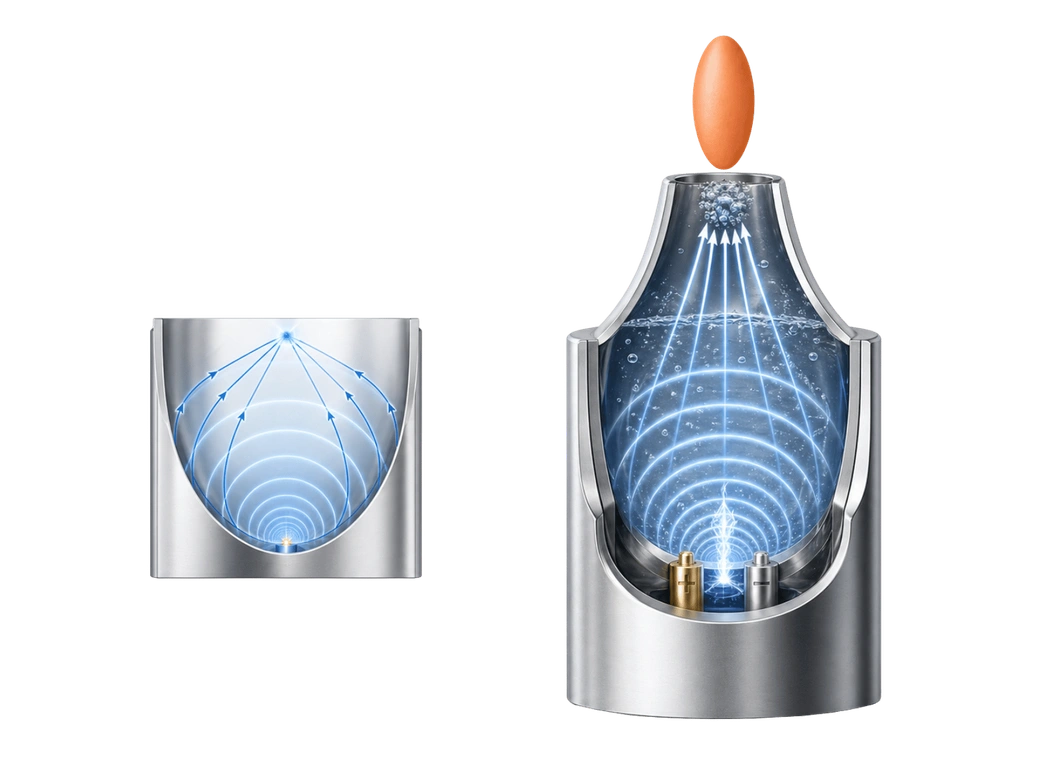
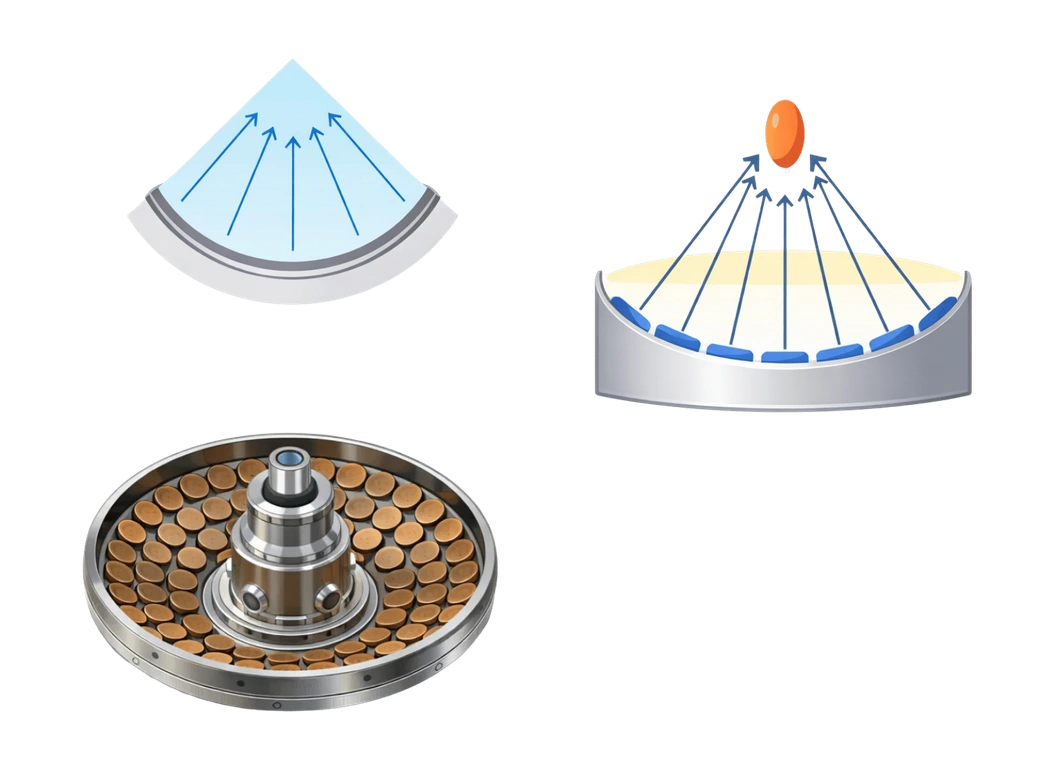
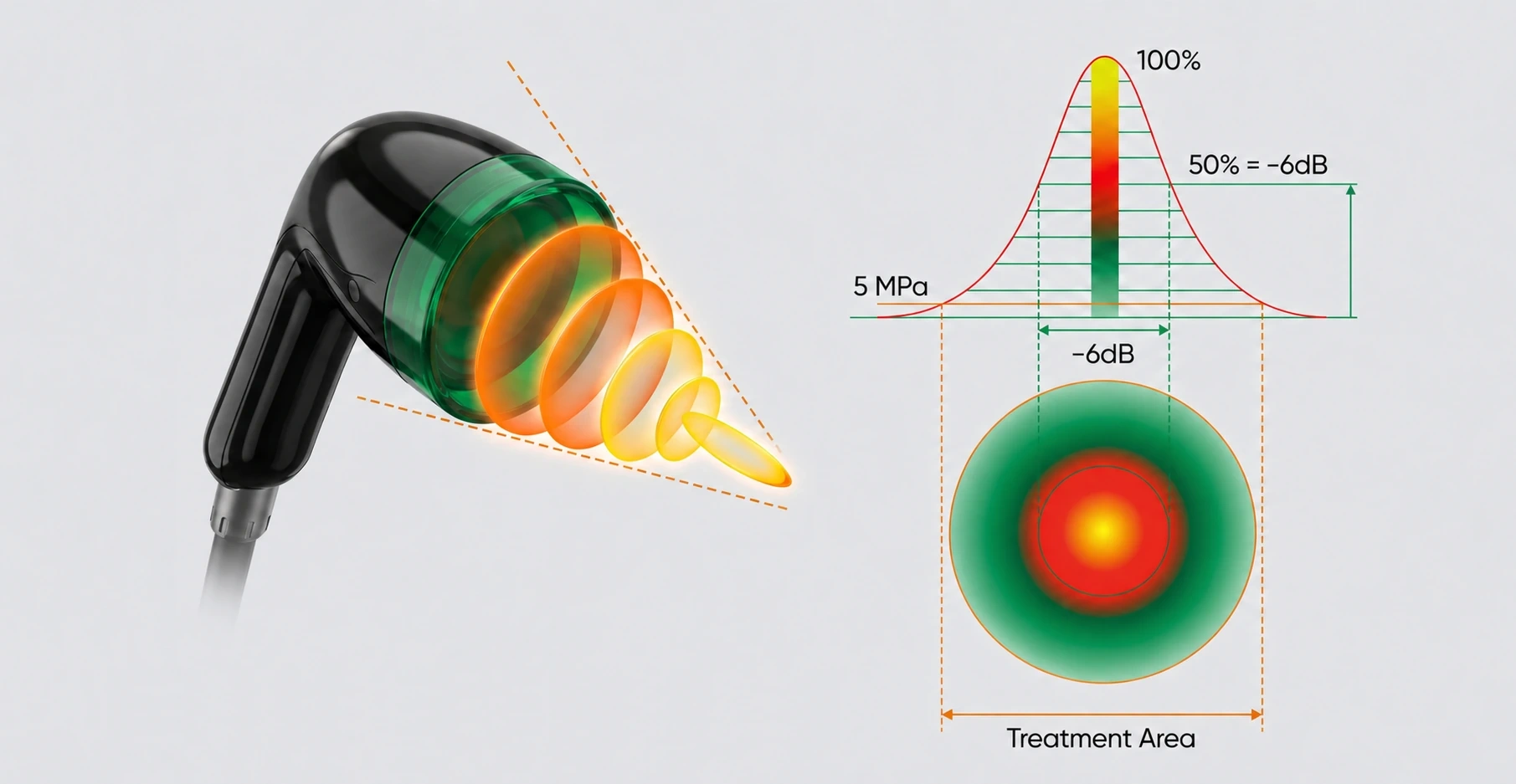
Action of the focused wave in a defined focal zone
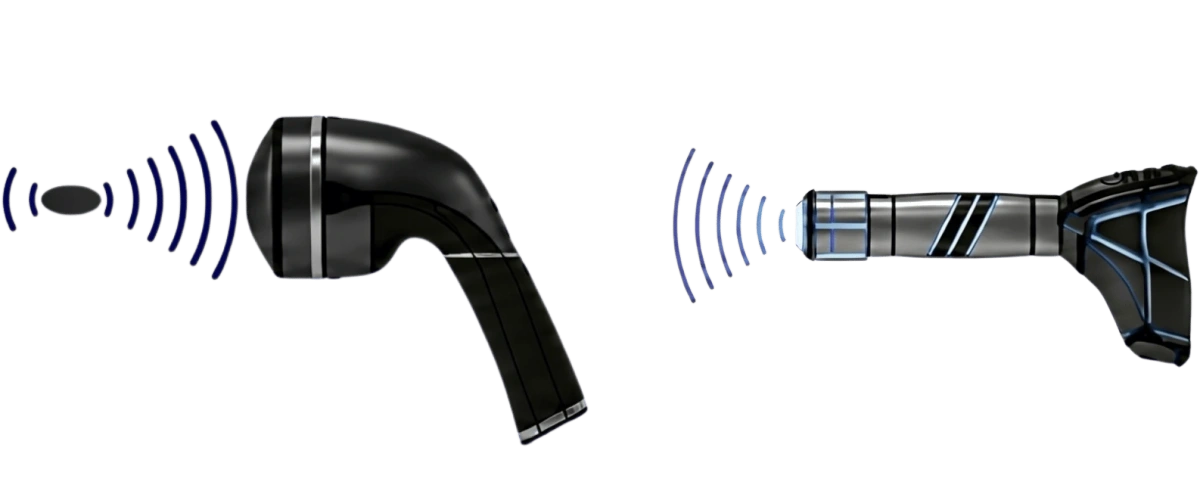
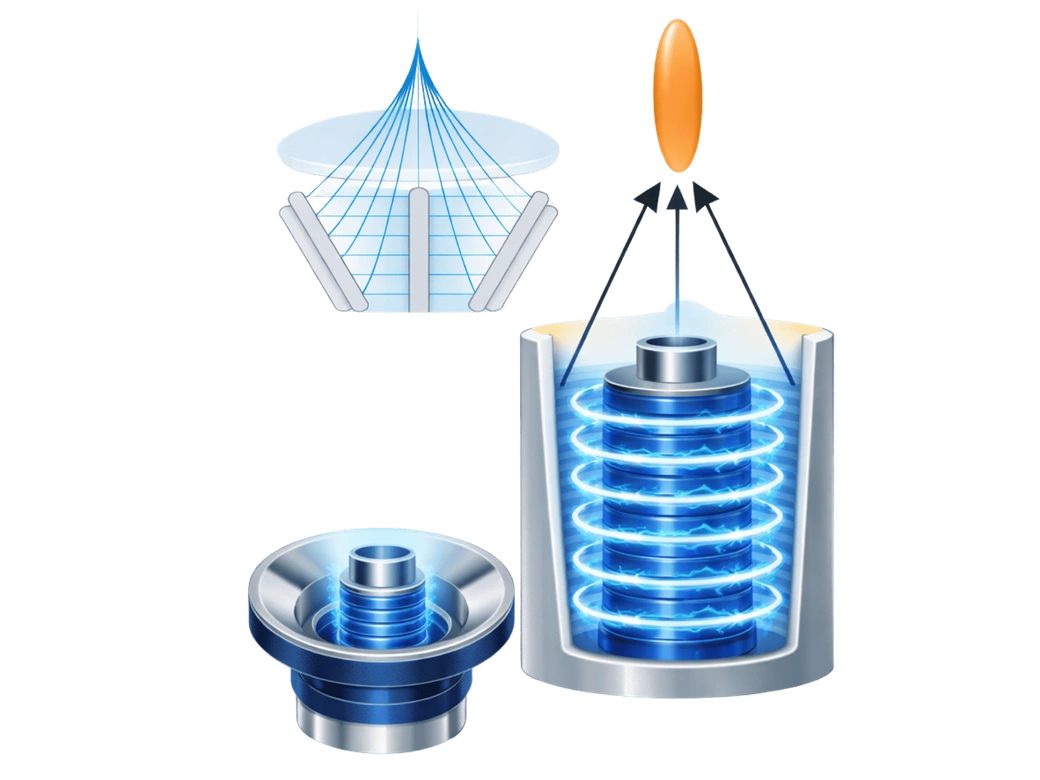
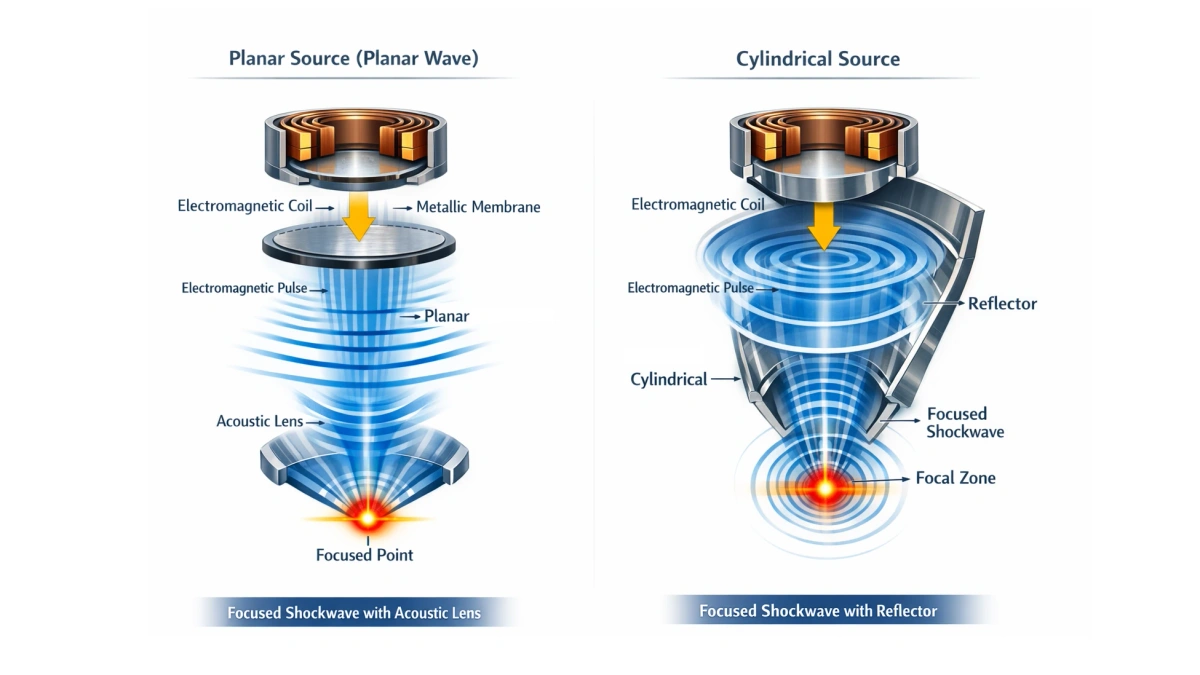
Focused shockwave therapy concentrates high-energy waves in a localized treatment zone. Compared with radial shockwave therapy, the focused technology directs mechanical energy toward deeper tissue layers and may help the healthcare professional reach target structures that are difficult to treat with surface-acting systems.
Key therapeutic properties
- High precisionFocused waves allow a localized mechanical action on tendons, ligaments, periarticular tissues and other deep anatomical structures within a defined focal zone.
- Treatment depthFocal depth is adjustable, while the therapeutic effect may extend beyond the focal zone depending on tissue properties and the selected physical parameters.
- Controlled tissue responseThe focused wave produces a localized mechanical effect that may support remodeling processes in target tissues under professional clinical supervision.