General chemistry panel I
TP (Total Protein) - total protein
Recovery
TP = total protein resource of the body
In sports, the total protein level is important for assessing recovery and the overall condition of the body.
ALB (Albumin) - albumin
Recovery
ALB = substance transport and protein status
Albumin is responsible for transporting substances in the blood, and its level helps assess the condition of the liver and kidneys. In athletes, a drop in albumin may indicate overtraining or insufficient nutrition.
GLO (Globulin) - globulins
Recovery
GLO = immune and inflammatory reactivity
Globulins play an important role in the immune system, and their level helps assess recovery after exertion and the inflammatory response of the body.
ALB/GLO (Albumin/Globulin Ratio) - albumin/globulin ratio
Balance
ALB/GLO = protein balance and inflammatory status
This ratio shows the balance between the main blood proteins. A reduced ratio may indicate inflammatory processes or changes in immune function.
ALT (Alanine Aminotransferase) - alanine aminotransferase
Liver
ALT ↑ = overload of the liver or muscle tissue
ALT is an enzyme used to assess liver function. In athletes, an elevated value may indicate muscle damage after intense effort.
AST (Aspartate Aminotransferase) - aspartate aminotransferase
Muscles
AST ↑ = muscle or liver damage
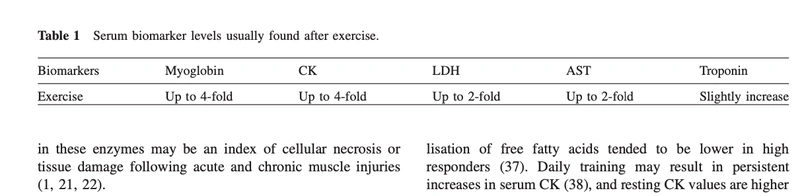
AST is also important for assessing the condition of muscle and liver tissue. In sports, an elevated AST value is usually associated with intense training and muscle damage.
TBIL (Total Bilirubin) - total bilirubin
Liver
TBIL = overall bilirubin metabolism
Bilirubin reflects liver function. In athletes, an increase may be related to altered hemoglobin metabolism from prolonged effort.
DBIL (Direct Bilirubin) - direct bilirubin
Liver
DBIL ↑ = biliary excretion and liver overload
An elevated direct bilirubin value may indicate changes in biliary or liver function, especially during intense effort.
IBIL (Indirect Bilirubin) - indirect bilirubin
Hemolysis
IBIL ↑ = breakdown of red blood cells due to exertion
Indirect bilirubin may rise due to increased breakdown of red blood cells, which is relevant for athletes with high aerobic loads.
TG (Triglycerides) - triglycerides
Metabolism
TG = lipid metabolism and nutrition
The blood triglyceride level helps assess cardiovascular risk, especially in athletes with a high-calorie diet.
CHOL (Cholesterol) - cholesterol
Metabolism
CHOL = lipid profile monitoring
Monitoring cholesterol values is important for maintaining cardiovascular health, especially in athletes with a high-fat diet.
HDL-C - high-density lipoprotein ("good cholesterol")
Cardiovascular risk
HDL-C ↑ = more favorable lipid profile
A high HDL value is beneficial for athletes, as it is associated with a lower cardiovascular risk.
LDL-C - low-density lipoprotein ("bad cholesterol")
Cardiovascular risk
LDL-C ↑ = risk of atherosclerosis
An elevated LDL value increases the risk of atherosclerosis. For athletes, it is important to keep LDL within the normal range.
GLU (Glucose) - glucose
Energy
GLU = energy availability for performance
Glucose is the main energy source. In athletes, glucose levels help assess availability for training and the risk of hypoglycemia.
CRE (Creatinine) - creatinine
Exertion
CRE ↑ = dehydration, muscle or renal overload
A marker of renal function. In athletes, elevated creatinine values may indicate overtraining or dehydration.
UREA (Urea) - urea
Catabolism
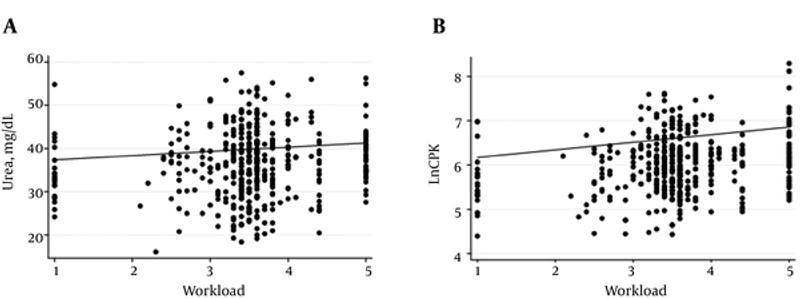
UREA ↑ = increased protein breakdown
An indicator of protein catabolism. Elevated values may indicate increased protein breakdown and insufficient recovery.
UA (Uric Acid) - uric acid
Exertion
UA ↑ = cellular breakdown and intense effort
An elevated uric acid value may indicate increased cellular breakdown during intense exertion.
Clinical emergency panel
AST (Aspartate Aminotransferase) - aspartate aminotransferase
Muscles
AST ↑ = sign of muscle damage after strength training
Important for assessing muscle tissue damage after strength training.
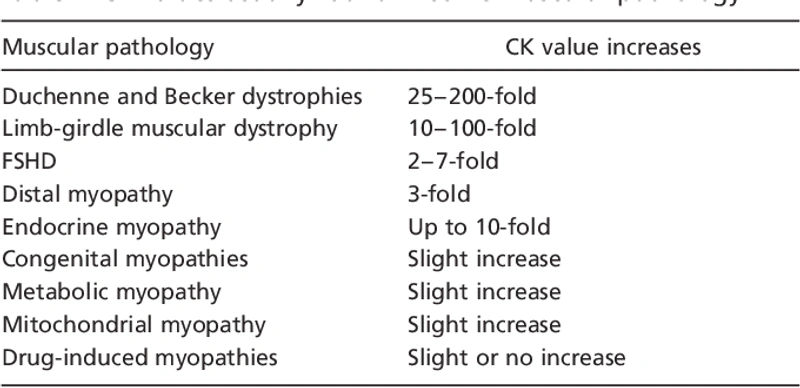
CK (Creatine Kinase) - creatine kinase
Muscles
CK ↑ = primary marker of muscle damage
A primary marker of muscle damage. Elevated CK values are seen after intense exertion and can serve as an indicator of overload, insufficient recovery, and increased injury risk.
CK-MB (Creatine Kinase-MB) - creatine kinase-MB
Heart
CK-MB = assessment of heart muscle
Specific to the heart muscle. It is used to assess heart muscle damage, which is especially relevant when cardiac problems are suspected after intense training.
LDH (Lactate Dehydrogenase) - lactate dehydrogenase
Muscles
LDH ↑ = tissue damage and high exertion
An elevated LDH value indicates cellular damage, both muscular and cardiac, which is important for assessing the athlete after intense effort.
α-HBDH (α-Hydroxybutyrate Dehydrogenase) - α-hydroxybutyrate dehydrogenase
Heart and muscles
α-HBDH ↑ = damage to cardiac and muscle tissue
A marker of damage to cardiac and muscle tissue. It can rise after prolonged exertion.
GLU (Glucose) - glucose
Energy
GLU ↓ = energy deficit during aerobic effort
Reflects the state of energy metabolism. A drop in level may be due to prolonged aerobic effort.
AMY (Amylase) - amylase
Metabolism
AMY = digestive and stress-related marker
Amylase may be elevated in response to physiological stress, dehydration, or digestive factors.
CRE (Creatinine) - creatinine
Exertion
CRE ↑ = muscle overload or renal stress
An elevated creatinine value may indicate muscle overload or kidney problems.
UA (Uric Acid) - uric acid
Catabolism
UA ↑ = intense cellular breakdown
An elevated value may be due to intense training that causes cellular breakdown.
K+ (Potassium) - potassium
Electrolytes
K+ = muscle contractility and cardiac function
Potassium is important for the functioning of the muscles and heart. Its values influence muscle contraction and recovery after training.
Na+ (Sodium) - sodium
Electrolytes
Na+ = fluid and electrolyte balance
Sodium regulates fluid and electrolyte balance. Sodium values can change in cases of dehydration, which is critically important for athletes training in warm climate conditions.
Cl- (Chloride) - chloride
Electrolytes
Cl- = acid-base and fluid balance
Chloride takes part in maintaining acid-base balance and body fluid balance, which is important for physical activity.
CO2 (Carbon Dioxide) - carbon dioxide
Acid-base balance
CO2 = acid-base balance
An indicator of acid-base balance. Relevant for assessing the athlete during high-intensity effort.